

Bill Gates, Kenya, and the “8-Year Contraceptive”: Fact, Innovation, and Controversy in Africa’s Reproductive Health Debate
An Introduction to a Discussion About a Recent Viral Story
In August 2025, the Bill & Melinda Gates Foundation announced a landmark financial commitment: $2.5 billion dedicated to women’s health research and innovation through 2030, with a stated focus on low- and middle-income countries. Buried within that announcement — and quickly amplified across social media — was news of a hormonal intrauterine device (IUD) designed to prevent pregnancy for up to eight years, now being rolled out across Kenya, Nigeria, and potentially India.
The last few months have seen an increase in the sharing of headlines and social media posts telling of Bill Gates, through the Bill & Melinda Gates Foundation, “Launching An 8-Year Contraceptive in Kenya”.
The claim has produced passionate responses ranging from excitement over a new medical solution to fears of past global health interventions and their effects on Africa.
So, what is the truth? Is this a significant launch, or just a misunderstanding due to the spread of false information?
What exactly is the “8-year contraceptive”?
The device at the centre of this debate is called Avibela — a levonorgestrel-releasing intrauterine system (LNG-IUS). It releases a synthetic hormone called progestin into the uterus continuously, preventing pregnancy for up to eight years.
The Gates Foundation’s role is financial and logistical. The Foundation states clearly that it does not manufacture or distribute contraceptives. What it does do is fund partner organisations — in this case, a US-based nonprofit called FHI 360 — which has been running a project called SHINE (Scale-up of Hormonal IUDs in New and Emerging Markets) across Kenya, Malawi, and Nigeria since 2022.
Anita Zaidi, President of the Gates Foundation’s Gender Equality Division, stated that a new hormonal IUD “designed for affordability and a user-centred experience” is being launched in Kenya, Nigeria, and possibly India. Medicines360, in partnership with DKT WomanCare, has signed deals to make Avibela available in these markets. Major procurement agencies including USAID and UNFPA have already added the device to their supply catalogues.
The Foundation says this is about closing the gap for an estimated 218 million women in low- and middle-income countries who have an unmet need for modern contraception.
That is the official position. Now let us go deeper.
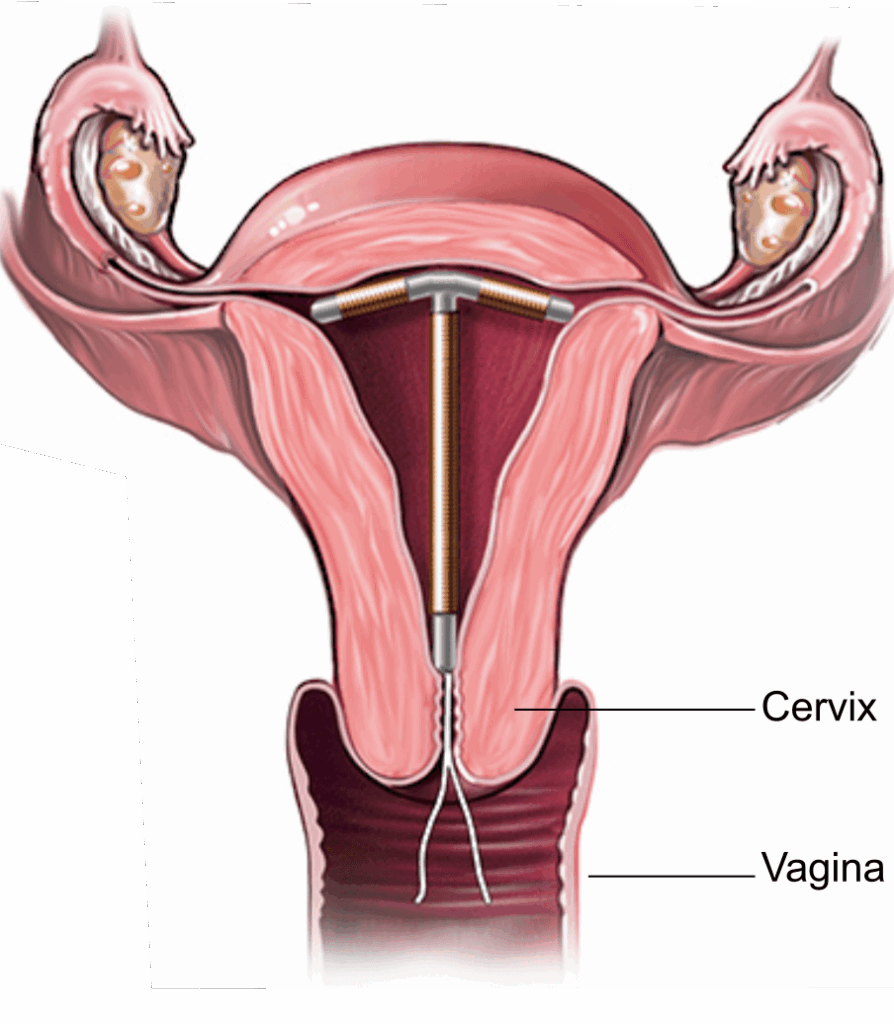
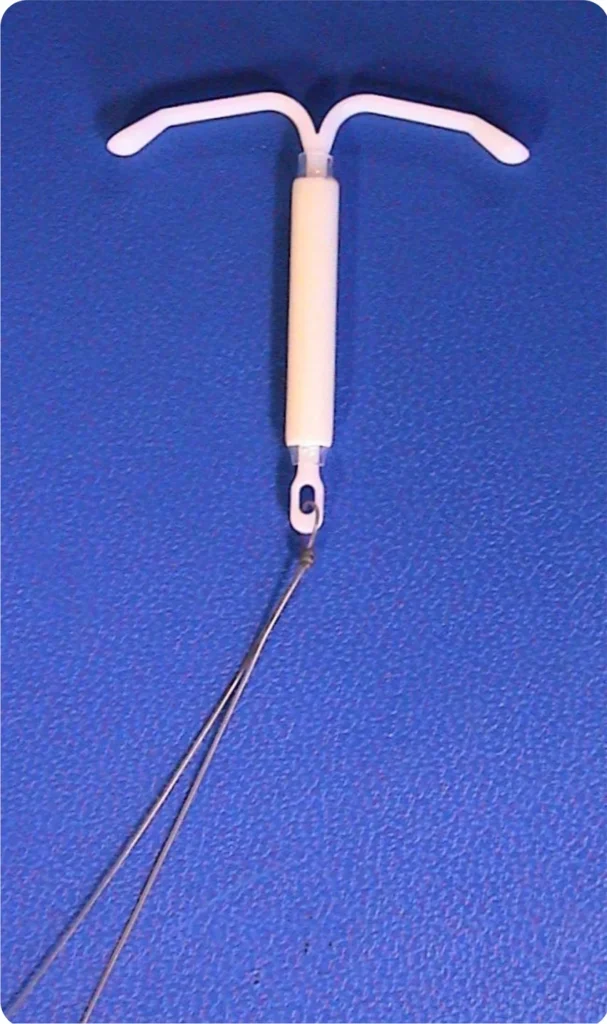
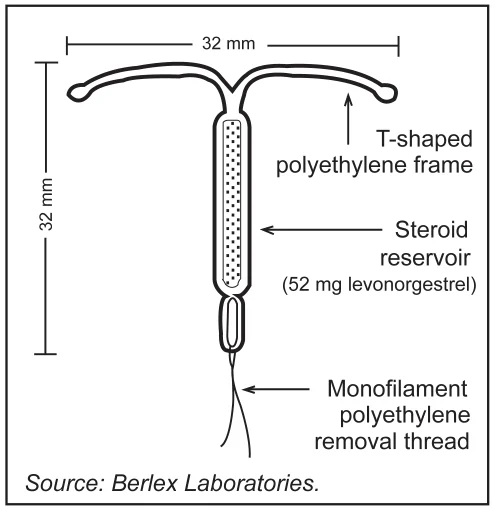
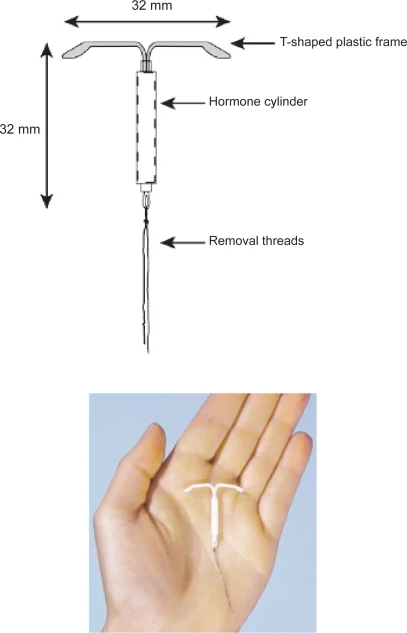
The method being discussed is a hormonal intrauterine device (IUD)—a small, flexible, T-shaped device placed inside the uterus by a trained health professional.
- It releases a low dose of progestin (levonorgestrel) over time
- Works by thickening cervical mucus and thinning the uterine lining
- Depending on the model, it can be effective for up to ~8 years
- It is reversible—fertility typically returns after removal
This type of contraception is already used globally; what’s changing is availability and duration labeling in some programs.
Progestins exert significant and complex effects on the endometrium, the inner lining of the uterus. These effects are central to both contraceptive mechanisms and the management of various gynecological conditions. The specific impact depends on the type of progestin, its dose, the delivery method, and the duration of use.
The Normal Endometrial Cycle and Progesterone’s Role
To understand the effects of progestins, it’s essential to first understand the natural role of progesterone. The menstrual cycle is divided into two phases:
- Proliferative (Follicular) Phase: Under the influence of estrogen, the endometrium grows and thickens. Glands lengthen, and blood vessels proliferate.
- Secretory (Luteal) Phase: After ovulation, the corpus luteum produces progesterone. Progesterone transforms this proliferative lining into a secretory, receptive state. It stabilizes the endometrial tissue, makes the glands secrete glycogen (to nourish a potential embryo), and decreases estrogen-driven proliferation. If pregnancy does not occur, progesterone levels fall, leading to menstruation.
How Progestins Alter the Endometrium
Progestins are synthetic analogs of progesterone. They bind to and activate progesterone receptors, mimicking and often amplifying progesterone’s natural effects. The primary actions on the endometrium are:
- Antiproliferative Effect: Progestins counteract the growth-promoting effects of estrogen. They inhibit endometrial cell proliferation, which is a key mechanism for preventing pregnancy and treating conditions like endometrial hyperplasia.
- Decidualization: Progestins induce decidualization, a process where stromal cells in the endometrium enlarge and transform into decidual cells. This creates a highly specialized, glandular-rich, and immune-modulated environment. While this is a normal part of early pregnancy, continuous progestin exposure creates a stable, decidualized state that is inhospitable to embryo implantation.
- Glandular Atrophy: With prolonged exposure, progestins cause the endometrial glands to shrink and become inactive (atrophic). This leads to a thin, flat endometrial lining.
- Altered Secretions: The composition of endometrial secretions changes, becoming less conducive to sperm survival, motility, and embryo development.
- Vascular Changes: Progestins affect the spiral arteries of the endometrium, leading to changes in blood flow and vessel stability.
Endometrial Effects by Progestin Delivery Method
The specific endometrial morphology varies significantly depending on how the progestin is delivered:
- Combined Oral Contraceptives (COCs): COCs contain both estrogen and a progestin. The estrogen component prevents significant endometrial atrophy. The progestin component leads to a “pseudo-secretory” or inactive state that is thinner and more stable than a natural cycle. This often results in lighter, more regular, and less painful menstrual bleeding.
- Progestin-Only Pills (POPs): The continuous, low-dose progestin leads to variable effects. It primarily thickens cervical mucus but also causes some degree of endometrial suppression, leading to unpredictable spotting or light bleeding in many users.
- Levonorgestrel-Releasing Intrauterine System (LNG-IUS, e.g., Mirena): This method produces the most profound local endometrial changes.
- Mechanism: The device releases a very low, continuous dose of levonorgestrel directly into the uterine cavity, creating extremely high local concentrations with minimal systemic absorption.
- Effect: This potent local effect causes profound glandular atrophy and stromal decidualization. The endometrium becomes extremely thin (often <4mm), inactive, and uniformly suppressed. This is why amenorrhea (absence of periods) or very light bleeding is so common with the LNG-IUS. This effect is completely reversible upon removal.
- Injectable Progestins (e.g., Depo-Provera): The high, continuous systemic dose of medroxyprogesterone acetate leads to significant and prolonged endometrial suppression, causing glandular atrophy. This results in amenorrhea in a large percentage of users after several months of use.
- Progestin Implants (e.g., Nexplanon): The continuous release of etonogestrel leads to moderate endometrial suppression. The effect is less predictable than with the LNG-IUS or injectables, often resulting in irregular bleeding patterns that can include spotting, prolonged bleeding, or amenorrhea.
Clinical Applications of Progestin Effects on the Endometrium
These effects are harnessed for several therapeutic purposes:
- Contraception: The suppressed, thin, and inhospitable endometrium prevents implantation, which is a secondary mechanism of action (the primary mechanisms are usually ovulation inhibition and cervical mucus thickening).
- Management of Heavy Menstrual Bleeding (Menorrhagia): The LNG-IUS is a first-line treatment for heavy bleeding. By inducing profound endometrial atrophy, it reduces menstrual blood loss by up to 95%.
- Treatment of Endometrial Hyperplasia and Endometrial Cancer: Progestins (both high-dose oral and the LNG-IUS) are the standard treatment for non-atypical and atypical endometrial hyperplasia and for early-stage endometrial cancer in women who wish to preserve fertility. The antiproliferative effect reverses the precancerous or cancerous overgrowth of the endometrium.
- Menopausal Hormone Therapy (MHT): When estrogen is given to manage menopausal symptoms, a progestin is added (in women with a uterus) to protect the endometrium from estrogen-induced hyperplasia and cancer.
Reversibility and Fertility Return
A critical point is that these endometrial effects are almost universally reversible. The endometrium has a remarkable capacity to regenerate. Once the progestin is stopped (or the IUD is removed), the influence of the woman’s own estrogen and, eventually, natural progesterone cycles take over. The suppressed, atrophic endometrium will typically return to a normal, proliferative state within one to three months, restoring normal cyclical changes and the ability to support a pregnancy. The idea of “irreversible” endometrial damage from progestins is not supported by the vast body of medical literature.
The Health risks Mainstream Medicine ACKNOWLEDGES
Beyond reversibility, the documented side effect profile of levonorgestrel IUDs raises questions that have not been adequately communicated to women, particularly in Africa.
Mental Health: Multiple large-scale studies have found troubling links between LNG-IUDs and psychiatric conditions. A Swedish register-based cohort study of over 703,000 women found that the LNG-IUD was associated with a 57% increased risk of depression. The risk was highest in adolescent women, reaching a 157% increased risk for teenage girls using the device as their first ever hormonal contraceptive. A separate Danish nationwide study found associations between LNG-IUS use and increased antidepressant use, first diagnosis of depression, and elevated risk of suicide attempts — with the highest relative risk of suicide attempts occurring among adolescents within one month of insertion.
A systematic review published in peer-reviewed literature concluded that despite variations in study quality, “many studies report psychiatric symptoms associated with LNG-IUDs, predominantly depression,” and stated that “counselling patients about these risks should be mandatory.”
Breast Cancer: A 2020 meta-analysis estimated that users of levonorgestrel-releasing systems had an increased breast cancer risk, with an odds ratio of 1.16 overall and 1.52 for women over 50. A separate nationwide study in Denmark and Sweden, conducted on 78,000 women, found a 40% increased risk of breast cancer among hormonal IUD users. Researchers noted the “absolute risk is small” but acknowledged this information is rarely foregrounded in pre-insertion counselling.
Other Documented Risks: According to the Mayo Clinic, levonorgestrel IUDs may increase the risk of ovarian cysts and have been associated with pelvic inflammatory disease (PID) — a serious infection of the female reproductive organs that can cause scarring and long-term infertility. The device can also, in rare cases, cause uterine perforation during insertion. Other documented side effects include acne, hair loss, weight changes, irregular bleeding, and in some cases, jaundice.
The 8-Year Question: Critics have raised a pointed question: if existing hormonal IUDs are already approved for up to 8 years in Western markets (brands like Mirena and Liletta), why is this being framed as a “new” and revolutionary launch specifically for Africa? The research on long-term effects beyond 5 years remains limited. As one analysis put it: “Eight years is a dramatically long lifespan for a single contraceptive device — far longer than most existing IUDs. That raises important questions: how thoroughly has this device been tested over that time span?”
The Political Context: Why Africa?
This is the question many Africans are asking, and it deserves a direct answer.
The Gates Foundation’s own FAQ acknowledges that an estimated 19% of women in sub-Saharan Africa have an unmet need for modern contraception. The Foundation frames this as a health equity issue — women in Africa deserve the same contraceptive access as women in London or New York.
Critics counter: why are long-acting reversible contraceptives (LARCs) — devices that work for years without requiring ongoing user action — being prioritised over short-term, user-controlled methods like pills or condoms? One review of family planning literature from 2000 to 2020 in sub-Saharan Africa found that such interventions tended to favour long-acting forms of contraception, and that many measured “success” by whether women chose to use these contraceptives — not by other outcomes such as whether women were fully informed and chose not to use them.
The historical shadow is long. The development of IUDs was, as Africa Check notes, “closely linked with population control and the eugenics movement.” Studies of LARC interventions globally have found patterns of practices that undermine informed consent, “especially for marginalised populations, involving a spectrum of subtle to direct coercion.”
Bill Gates himself has spoken publicly about population growth in Africa, warning in a 2018 interview that Africa’s population projected to double by 2050 could put “hard-won progress in reducing poverty” at risk. The question being asked across the continent is: when a man who has spoken about population growth funds the mass rollout of 8-year contraceptives in Africa, can the two things truly be separated?
The Foundation insists they can. It states it is “deeply committed to the principle that all women have the right to make informed, voluntary choices about their reproductive health” and funds oversight mechanisms to prevent coercive use.
Namibia’s President Netumbo Nandi-Ndaitwah — the country’s first female president — was reported to have rejected proposals for IUD trials in her country, reportedly stating: “Namibia is a nation of modest size, with a population of just over 3 million. If any country should consider measures to curb population growth, it ought to be nations like the United States, with over 347 million people.” (Note: fact-checkers have flagged that the specific wording of this reported statement lacks verified primary sourcing and should be independently confirmed.)
Popular Kenyan men’s influencer @amerix argued on X that Kenya was “not overpopulated” and accused the government of blindly adopting unnecessary medical solutions championed by foreign actors. His post received over 217,000 views.
The Consent Question
At the heart of this debate — beyond politics, beyond the Foundation’s billions — is a simple, human question: are African women being told the full truth before this device is inserted into their bodies?
From a purely medical standpoint, informed consent for LNG-IUDs should include disclosure of:
- Documented links to depression and suicidality, particularly in younger women
- The increased breast cancer risk findings
- The risk of pelvic inflammatory disease and potential long-term fertility complications
- The requirement for a trained healthcare provider to remove the device — and what happens if that provider is not available
- The lack of long-term safety data specifically for 8-year use
Women in rural Kenya, Nigeria, and other targeted regions often have less access to healthcare literacy resources, less access to alternative contraceptive options for comparison, and — critically — less access to removal services if they change their minds or experience side effects.
A programme championed as empowering women must grapple honestly with these structural realities. Empowerment requires genuine, informed choice — not just the insertion of a device.
What The Foundation Says
In response to the controversy, the Gates Foundation has maintained several positions:
- It does not launch, manufacture, or distribute contraceptives directly.
- The $2.5 billion commitment is broad, covering five areas of women’s health — contraception is one part.
- Governments, not the Foundation, decide which health products to adopt.
- All its work is grounded in voluntary, informed consent principles.
- The 8-year hormonal IUD is not new — similar devices have been used in Western countries for years.
On that last point, the Foundation is correct on the technology. But the question of whether those devices have been adequately studied over 8 years, and whether the full side effect profile is being transparently communicated in rollout countries, remains open.
The Bottom Line
This is not a simple story of good intentions versus conspiracy. It is a complex story about power, bodies, money, consent, and the right of African women to make fully informed decisions about their own reproductive health.
The Gates Foundation is the most powerful private health funder on earth. Its decisions shape what medicines are developed, what get distributed, and where. That power deserves scrutiny — not because of what is imagined, but because of what is documented.
The health risks of levonorgestrel IUDs are real, published in peer-reviewed journals, and not widely communicated. The historical context of population-control programmes targeting African and Asian nations is real. The structural barriers that prevent African women from freely choosing to remove a device they regret are real.
And the 218 million women across low- and middle-income countries who lack access to reliable contraception — their need is also real.
What African women deserve is the full picture: every benefit, every risk, every political context, and the genuine freedom to say yes or no. Not a programme designed in Seattle, funded by billions, and delivered to their bodies without their full and meaningful consent.
That is the conversation Africa must have. And it must have it now.
EyeAfrica Investigations Desk. All figures and studies cited are drawn from published peer-reviewed literature and publicly available statements. Readers are encouraged to independently verify all claims and seek professional medical advice before making any reproductive health decisions.
